1049
Views & Citations49
Likes & Shares
Object: This
retrospective study was undertaken to define the prevalence of cavernous
malformations (CM) or CM-like lesion in children with medulloblastoma who were
postoperatively treated with radiation therapy (RT). We also aimed to clarify
the natural history of radiation induced CM or CM-like lesions.
Methods: The authors
reviewed medical records of 37children with medulloblastoma, who underwent
surgical resection, chemotherapy and RT during the period of 2002 to 2010. RT
was applied with cumulative doses ranging from 5400-5860cGy to the primary
posterior fossa with cranio-spinal axis doses <2340 cGy or >2340 cGy
depending on tumor staging. The patients were consecutively followed with
magnetic resonance (MR) imaging that included the 1.5 T or 3 T MRI modalities.
The diagnosis of CM or CM like lesions was done based on four-tier Zabramski
classification (Type I – IV).
Results: Thirty seven
patients were followed up for 5.2 years on average (SD 2.5 years). Among 37
patients, who received RT, 8 patients (21.7%) did not develop any cavernous
malformations. Mean age at the time of radiation therapy was 9.2 years (SD: 4.7
years). Twenty seven patients had type IV (dot-like CM) lesions and the
remaining two patients developed the type I. There were no type II or III in
this series. Only one of the type 1 developed symptoms (seizures) referable to
the cavernous angioma which was surgically removed. Latency interval between radiation therapy
and the development was 2.7 years on average (SD: 1.45 years). Even though type
IV or dot-like CM location occurred in any location in the brain, majority of
the lesions could be detected in the white gray junction in the cerebrum. Both
type I lesions were detected in the cerebrum. Ten patients had the one to three
lesions, 14 had four to six lesions, 3 had seven to nine lesions and 2 had more
than 10 lesions. Histology of two dot-like CM of type IV at autopsy showed
telangiectasia.
Conclusion: The development
of dot-like CM is quite common after RT for medulloblastoma in childhood. GRE
weighted images were superior to conventional T1-, T2- weighted images in
detection of CMs and CM-like lesions. The SWI weighted images were
statistically significantly superior to GRE weighted images in detecting
dot-like CM affecting both supratentorial and infrantentorial compartments.
These dot-like lesions are mostly clinically silent telangiectasia, and rarely
progress to hemorrhagic cavernous angioma.
Keywords: Cavernoma,
Medulloblastoma, Radiation therapy
INTRODUCTION
Radiation therapy (RT) is an integral part of the treatment of
pediatric patients with malignant brain tumors. In recent years, use of this treatment modality
contributed to longer patients’ survival but also underscore the importance of
awareness of long-term complications caused by RT and how they might affect
patients’ management during extended periods of observation.
Well-known early and late complications of RT
such as brain atrophy, white matter necrosis, edema, demyelination, dystrophic
mineralization and vascular abnormalities were described extensively in the
past [1,2].
Vascular complications are late sequels of RT
and theyinclude cerebrovascular
accidents, lacunar lesions, vascular occlusive disease including
moyamoya syndrome, hemorrhage and vascular malformations. [3,4]. Vascular
malformations are represented by telangiectasia, cavernous malformation (CM)
and aneurysm. Little is known how telangiectasia and CM occur and how they are
linked together.
There are several reports
in the current literature related to the development of post-radiotherapy CM
but only few publications of cerebral dot-like cavernous malformations can be
found [5-9]. Rigamonti et al reported that capillary teleangiactasia and
cavernous malformations are a spectrum within a single pathological entity [10]. Zabramski classified the same telangiectactic changes
previously reported by Rigamonti et al. into type IV changes in his four tier
classification system of cerebral cavernous malformations [11].
The aim of this study is to
describe the incidence of dot-like cavernous malformations in pediatric
population of patients with medulloblastoma who underwent chemo and radiation
therapy.
MATERIAL AND METHODS
We retrospectively reviewed
a cohort of 45 children with medulloblastoma, postoperatively treated with RT
and chemotherapy at a single institution in order to elucidate the
pathophysiology of the natural history of dot-like cavernous malformations and
cavernous malformations. This group of patients underwent frequent magnetic
resonance (MR) imaging follow up for the detection of recurrent tumor and
gradient echo sequence (GRE) or susceptibility weighted imaging (SWI) were part
of the established follow up imaging protocol intended to identify
possible radiation induced late effect such as radiation-induced CM.
The brain tumor database at
the Ann & Robert H. Lurie Children’s Hospital of Chicago was reviewed to
retrieve the data between 1 January, 2002 and 31, December 2010 and to identify
all the patients with medulloblastomas, who underwent surgical resection,
followed by radiation and chemotherapy and who have undergone the long-term
imaging surveillance at this single institution.
Institutional Review Board
approval (IRB#2005-12692) was obtained prior the retrieval of clinical and
radiographic data. All patients were diagnosed before 18 years of age, and had
long-term MR imaging surveillance. A retrospective charts review was performed
and patients’ clinical and demographic data were collected. All patients were
followed clinically and radiologically at different intervals, beginning at 3
months postoperatively with follow up radiological examination repeated every 3
for the first 2 year, then every 4 to 6 months till the 5th year,
then yearly depending on status of the disease.
Preoperatively every
patient obtained the MR imaging studies of the head on 1.5 T or 3.0 T magnet.
The imaging included T1-, T2-, GRE, SWI and triplanar post gadolinium
contrasted T1 weighted.
Neuro-imaging studies were reviewed for the
presence, number, size, and anatomic location of dot-like cavernous
malformation and CM. Follow up MR
imaging studies were also obtained on a 1.5 T and/or 3.0 T magnet, and included
axial T1-, T2-, and GRE, SWI and triplanar post gadolinium contrasted T1
weighted images.
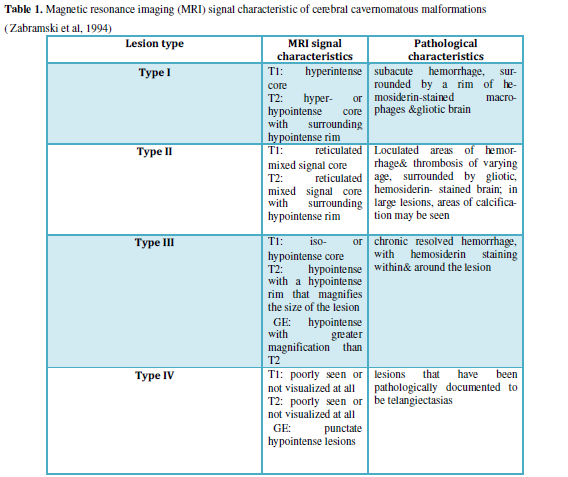
The diagnosis of CM was
done based on four-tier Zabramski classification; Type I-III are visible on at
T1-, T2-weighted imaging [11], whereas Type IV, the
dot-like cavernoma-like lesion, is visualized only on GRE or SWI weighted images (Table 1). Pathology review of the specimens from two autopsies was
completed for evaluation of dot-like cavernoma.
Statistical analysis was
done with the use of SPPS 11 software, and statistical significance was defined
as p value < 0.05.
RESULTS
Between 2002 and 2010, a total of 45 patients
(28 male and 17 female) with medulloblastoma had surgical resection for their primary tumors at our institution.
Out of 45 patients, 37 received both RT and chemotherapy, and were included in
the study cohort for further analysis. None had familiar history of
cavernomatosis. Of these 37 patients, 5 received proton beam therapy with
cumulative dose of 54GyRBE and the remaining 32 received standard external beam
RT with cumulative doses ranging from 5400-5860cGy to the primary posterior
fossa site. To the cranio-spinal axis with doses ranging from 23.6 GyRBE to 36
GyRBE by Proton or 2340 cGy to3600 cGyby external beam RT depending on tumor
staging.
At the initial tumor presentation, preoperative
MR of the brain did not reveal CM in any patients. The surveillance
neuro-imaging in this study included the 1.5 T or 3 T MRI. Thirty seven
patients were followed up radiologically and clinically for 5.2 years on
average (SD 2.5 years).
Among 37 patients, who received RT, 8 patients
(21.7%) did not develop any CMs. However, the mean follow up period was short,
2.8 years SD 2.7 years) among this cohort. Among this group -7 patients
received standard external beam RT and 1 patient received proton beam therapy.
Furthermore, 4 patients in this cohort did not have sufficient length of
observation period because of the disease progression and early death within
couple of months following completion of RT. Another patient transferred to
another institution for the follow up care after RT and, subsequently, was lost
to follow up. Mean age at the time of RT was 9.2 years with standard deviation
(SD) of 4.7 years. The latency interval between the completion of RT and the
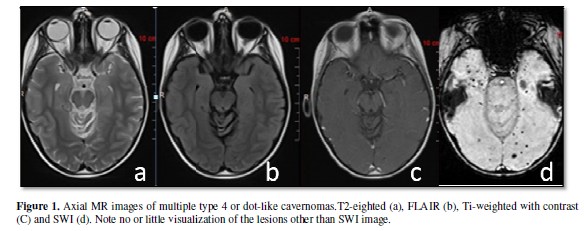
development of CMs or CM-like lesion was 2.7 years (SD: 1.5years). MR imaging
revealed Zabramski type IV lesions (dot-like cavernoma) in all except for 2
(Figure 1).
Among those 29 patients with type IV or
dot-like lesions, 5 patients had CM lesions in both supratentorial and
infratentorial areas. Even though dot-like lesions occurred anywhere in
multiple locations of the brain, majority of the lesions were detected in the
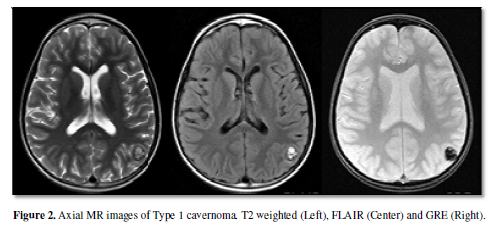
white-gray junction or white matters in the cerebrum. The numbers of the CM
lesions were as follows: 10 patients had one to three lesions, 14 had four to
six lesions, 3 had 7 lesions and 2 had greater than 10 lesions (Figure 2).
The number of the lesions may increase the first 6 to 18 months after detection
but subsequently they become stabilized.
Two patients had type I lesion. Only one of them developed symptom: he
had sudden onset of seizure due to a lesion in left temporal parietal region
and because of persistent nature of seizures he was subjected to surgical
resection (Figure 3). This patient
had only solitary cavernous angioma.
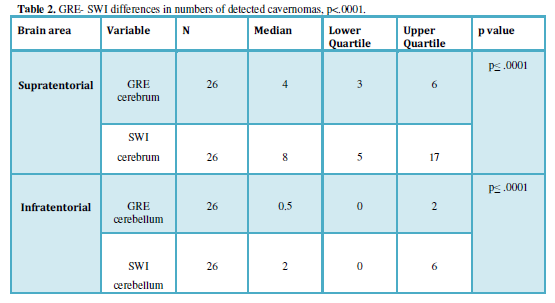
Both GRE and SWI weighted images were superior to conventional T1-, T2- weighted images
in detection of cavernous malformations. SWI is a 3D high-spatial resolution
fully velocity corrected GRE. Both are sensitive to detect compounds of
paramagnetic, diamagnetic and ferromagnetic properties. However, the SWI weighted images were
statistically significantly superior to GRE weighted images in detecting
dot-like cavernous malformation in supratentorial and infrantentorial
compartments. We had 26 instances where both GRE and SWI sequences were recorded.
These were compared using Mann-Whitney non-parametric test and significant
differences were found in numbers of cavernomas in both infratentorial and
supratentorial areas (p≤ .0001) (Table 2).
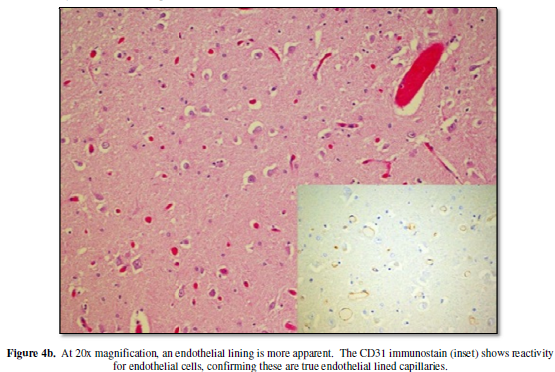
Two patients who developed multiple dot-like cavernous malformations
died during follow up due to medulloblastoma progression. The brain of those
two patients harvested at post-mortem examination was subjected to pathological
examination. Pathology findings revealed dilated thin-walled vessels with scant
intervening brain parenchyma showing reactive gliosis and hemosiderin-laden
macrophages. An EVG stain shows no evidence of internal elastic lamina in the
vessels. These findings are compatible with telangiectasia (Figure 4a, 4b).
Seven patients died of the progression of
medulloblastoma; 3 early death as mentioned above and additional 4 patients 2.5,
4, 4 and 9 years after RT. One patient
was lost to follow up. All other 29 patients are alive from 5 to 13 years at
the time of writing.
DISCUSSION
Cerebral CMs comprise 5%-13 % of all central
nervous system vascular malformations with estimated prevalence in general
population of 0.3-0.5% [12,13]. CM are blood cavities that are characterized by closely packed, thin
wall enlarged vessels, lined by a single layer of endothelial cells without the
muscular tissue or intervening brain parenchyma. CM areoccult vascular lesions
of the brain, and they are most commonly asymptomatic, but they might present
with sudden onset of headache, seizure, hemorrhage or focal neurological
deficit due to mass effect. The estimated risk for cerebral CM hemorrhage is
3.1 % per year and for seizure is 2.4% per year [14].
Cerebral CMs occur most commonly as sporadic lesions, and then patients usually have only one malformation. CM also might occur in familiar form, when few family members are affected, and then patient’s presents with multiple cavernousmal formations. Familial cases follow an autosomal dominant mode of inheritance and are caused by mutations in CCM1 (KRIT1), CCM2 (MGC4607), or CCM3 (PDCD10) genes. Somatic mutations within the three CCM genes have been identified in CM lesions from both sporadic and familial patients. As 5 to 15% of familial CM cases remain still genetically unexplained [15].
Cranial
radiation is main integral part of treatment for brain tumors, solid tumors of
the head, and disorders with the involvement of central nervous system (CNS)
such as brain metastases, and in cases when prevention of relapse of acute
leukemia is warranted. Complications of the brain RT are well known and are related to
the dose, fraction, and volume of irradiated brain, patient age, and
concomitant therapy. According to the time of appearance we can divide the CNS reaction to the radiation
to: 1) acute reactions that occurs during current radiation; 2) early delayed
reactions, which appear from few weeks to 2 to 3 months after end of radiation
therapy; and 3) late delayed reactions that can be manifested months to years
after completion of the therapy [16].
Arteries
and capillaries are especially sensitive to the radiation injury with veins
being more resistant. It was shown in an animal model that approximately
15 % of endothelial blood vessel cells were lost within 24 hours after
radiation with dose of 5-200 Gy [17], The direct consequence of radiation
vasculature damage is a disruption of blood- brain barrier that causes
vasogenic edema and tissue hypoxia. The endothelial loss is followed by thrombi
formation and hemorrhage [18].The vascular injury will lead to endothelial proliferation of injured
vessels and formation of new vessels, basal membrane thickening, fibrosis of
adventitia of blood vessels, and vessels dilation [19].
Many
pro-inflamatory genes are upregulated within hours after radiation exposure
such as tumor necrosis α, interleukin-1β and nuclear factor-kappa B [20]. Due to tissue hypoxia vascular
endothelial growth factor (VEGF) is also elevated and has direct effect on
development of new blood vessels [21].
Degree of
the damage of the brain vessels is dose dependent and lower doses of radiation
might not cause initial vessel damage. The effect of low radiation dose can be
delayed 1-2 years after radiation exposure and can present with hemorrhagic
infarct and telangiectasia formation [22,23].
Gaensler
et al. published in 1994 their case series of 16 patients who underwent the
whole brain irradiation as part of treatment protocol of primary brain tumors,
with 14 patients being younger than 18 years old at the time of irradiation,
who developed focal hypointense lesions on T2-weighted MRI images. Pathological
examination of 6 patients with these lesions revealed small to larger regions
of acute hemorrhage and revealed numerous thin-walled, ectactic vessels among
normal neuropil elements. These lesions were considered to be telangiectactic
changes [22].
Brain
telangiectasias are dilated capillaries with thin endothelial walls, and are
asymptomatic lesions of the brain with low vascular flow. Koike and al.
followed 90 pediatric patients with the brain tumor who received RT with median follow up of 8.1 years
with the MR. They found that 20 % of the patients developed telangiectactic
changes and great majority was in the group who received more than 32 Gy of
radiation. Half of the patients continued to develop additional new
telangiectactic lesions 5 years after radiation [7].
First
report of spontaneous hemorrhage, that developed in pediatric patients with
brain tumors several years after craniospinal irradiation at the site away from
brain tumor and revealed abnormal blood vessels in two of three patients, has
been published in 1991 by Allen et al. [24]. Several years later Cirillo et al. [25] reported seven cases of cerebral
CM in pediatric patients with brain tumor after craniospinal irradiation, with
one patient that required surgical removal of hemorrhagic CM. Subsequently many other case
studies and two-literature review of radiation-induced CMs, with review of 85 and 72 cases
respectively, have been published [26,27].
Zabramski
et al. classified CMs into four-tier classification according to their histological and MR
features [11]. Type I
malformations are characterized by hyperintense core on T1 and hyper- or
hypointensity core on T2-weighted sequences. In type II malformations, CMs
exhibit a core with reticulated mixed signal intensity on T2-weighted sequences
and on T1-weighted images, with a well-circumscribed hypointense rim on
T2-weighted sequences. Type III malformations show a iso- or hypointensity on T1-weighted
sequence and a hypointensity on T2-weighted sequence as well as a rim that is
hypointense on T2-weighted sequences. Type IV malformations are punctate
hypointense lesions on T2- weighted GRE MRI. Pathologic evaluation of the type
I malformations revealed cavernoma that are consisted of subacute hemorrhages,
type II malformations had hemorrhages and thrombosis of varying ages, and type
III malformations had chronic hemorrhages with hemosiderin within and around
the lesions. The pathology of type IV malformations can
represent capillary telangiectasias or a CM in an early stage. Our two cases of
brain autopsy of MR dot-like lesions on SWI sequence are confirming the theory
of telangiectasias as type IV malformations.
Our data
analysis shows that MR imaging is the best technique for evaluation of these
occult vascular lesions. Cavernomas are best detected on T2 and GRE weighted
images because of increased concentration of deoxyhemoglobin and hemosiderin.
Increased concentration of deoxyhemoglobin is due to slow blood flow through
cavernoma that leads to blood stagnation in the cavernas of the CM and
increased extraction of the oxygen from the blood. Increased deposits of
hemosiderin are due to microhemorrhages in and around CM. The hemosiderin deposits
within and around the lesion together with susceptibility changes between
deoxygenated blood and the surrounding brain tissue are causing signal loss
that can be easily detected with GRE and SWI weighted sequence. Type III and
type IV CM can be easily missed on conventional T1- and T2-weighted images [28, 29].
Detection
of cavernomas also depends on the strength of the magnetic field, thickness of
the section, and orientation of the section. Gold standard for detection of the
cavernoma is still T2 and GRE weighted images. CM have typically “popcorn’’ or
“mulberry’’ appearance with thin peripheral rim of decreased signal due
hemosiderin deposit in the surrounding brain parenchyma [28,30].
The Zabramski classification published in 1994 [11]
did not include the SWI in detection of CM lesions because SWI was introduced
in 1997. Most recently many papers showed that SWI is more specific and
sensitive for detecting dot-like cavernous malformations in familial cavernous
malformations. [30,31]. Our results also clearly showed that SWI is more
sensitive for detecting RT induced dot-like cavernous lesions. Initially the
lesions seen only on SWI were considered independently of the Zabramski
classification system, but based on our research and pathology review findings
that dot-like lesions correspond with the telangiectactic changes, we suggest
that use of SWI technique warrants the update of Zabramski classification and
recommend SWI as modality for detection of type IV lesion, since this method is
more sensitive for small lesions that can be easily omitted with GRE sequence.
Measuring
the diameter of the CM is possible only on T1- and T2 weighted imaging
sequence, but the lesion diameter of the dot-like lesion is still clinical
dilemma, since the appearance of the dot-like lesions is based on
susceptibility artifact of the lesion that is proportionally dependent on the
amount of hemosiderin deposit and technical aspect of the image acquisitions.
So it is not advisable to measure the size of the lesion on SWI weighted
imaging sequence.
Most
recent study by de Champfleur et al. showed that dot-like cavernomas are best
appreciated on the SWI weighted images; their numbers are significantly higher
with SWI then with the T2 weighted images [32].
SWI is a
technique that maximizes the sensitivity to susceptibility effects by combining
a long-TE high-resolution fully flow-compensated 3D GRE sequence with filtered
phase information in each voxel [29].SWI has an exquisite sensitivity to the venous vasculature, blood products,
and vascular malformations. Studies have suggested that SWI is more sensitive
than T2-weighted imaging for evaluating CM [30,31].In
de Souza et al. series of familial CM SWI showed 73% more lesions than T2-weighted GRE
images [30], and that was confirmed also by work of Bulut
et al. [31]. In our series we have showed that
the SWI was superior for detecting post radiation CM in both supratentorial and
infratentorial parts of the brain tissue.
Yamasaki
et al. [34] reported recently that of 25 patients with embryonal tumors (17
medulloblastomas, 5 primitive neuroectodermal tumors (PNET), 3 pineoblastomas)
treated with craniospinal irradiation, 18 were alive and free of the
recurrence. 14 patients developed CM in the course of a median of 56.7 months; 13 of these presented with
multiple CMs. Patients who
underwent RT at an age
younger than 6 years developed multiple CMs significantly earlier than those
treated at a later age (p = 0.0110). They found 4 patients with PNET/ pineoblastoma developed type 1 or 2 CM and significantly earlier than did 2 medulloblastoma patients
(p = 0.0042) [34]. Our analysis of 37
medulloblastoma cases treated with RT revealed that earlier age at time of
radiation therapy leads to more significant post-radiation damage of the brain
Average age at time of radiation leading to the development of type I lesions
is 7.2 years old (SD: 4.4 years) versus 9.2 years old (SD: 4.0 years) leading
to the development of Type IV lesions.
CONCLUSIONS
Although post RT dot-like CMs or telangiectasia rarely
cause symptoms like ours and others [6], they are common after RT for pediatric
brain. Younger the patients when they receive RT, the higher the tendency of developing CMs. Advances in RT such as reduction of the
radiation volume, new radiation protocols, use of proton beam therapy along
with advent of new therapeutics such as bevacizumab (anti- VGEF agent) might
cause less radiation related changes. Future studies might give us an answer if
the new therapies might have less detrimental long-term effect on brain blood
vessels, but this still needs to be elucidated.
DISCLOSURE
The
authors report no conflict of interest concerning the materials or methods used
in this study or the findings specified in this paper.
ACKNOWLEDGEMENT
We are
grateful to Karen Rycklik, MS, from Biostatistics Research Core, Stanley Manne
Children’s Research Institute, for her help and guidance with statistical
analysis of data.
-
 Table 1
Table 1 -
Table 2


QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- BioMed Research Journal (ISSN:2578-8892)
- Journal of Infectious Diseases and Research (ISSN: 2688-6537)
- Journal of Rheumatology Research (ISSN:2641-6999)
- Chemotherapy Research Journal (ISSN:2642-0236)
- Advance Research on Endocrinology and Metabolism (ISSN: 2689-8209)
- Journal of Allergy Research (ISSN:2642-326X)


